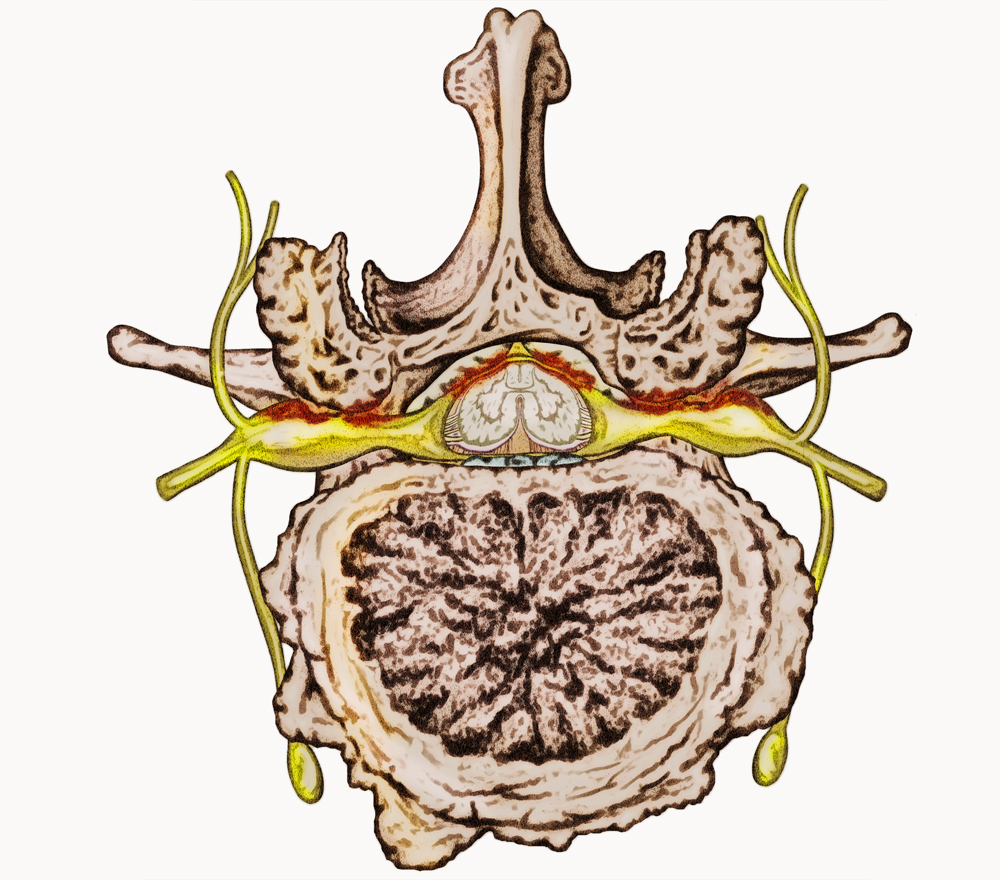
 The spine is made up of 33 vertebral bones. Each the bones has a large central canal opening for the spinal cord. Additional openings on each side of the spinal cord called foramens allow the exiting nerves to branch out from the spinal cord to the arms, legs and other parts of the body. The foramen is the space where the exiting nerve exits formed by two facet bones (facet Joint) above and the disc between the vertebral bodies below the exiting nerves.
The spine is made up of 33 vertebral bones. Each the bones has a large central canal opening for the spinal cord. Additional openings on each side of the spinal cord called foramens allow the exiting nerves to branch out from the spinal cord to the arms, legs and other parts of the body. The foramen is the space where the exiting nerve exits formed by two facet bones (facet Joint) above and the disc between the vertebral bodies below the exiting nerves.
What Causes Foraminal Stenosis?
Normally nerve roots have enough room to exit the spinal canal through the foramen. However, with age, degenerative disc disease and trauma, the foramen can narrow and compress the spinal cord and or exiting nerves. Some other conditions such as bulging or herniated discs, calcified ligaments and bone spurs and spinal arthritis may further affect the foramen. This condition can develop anywhere in our spine from cervical to thoracic and is most common in the lumbar region. The average age of patients suffering from spinal and foraminal stenosis is 55 years of age. The disease may affect women and men of varying ages and physical activity levels.
The patients at highest risk for stenosis are:
- Obese
- Smokers
- Sedentary lifestyle
- Lacking proper nutrition
What are the symptoms of Foraminal Stenosis?
Compression on the spinal and exiting nerve leads to inflammation which produces many different types of symptoms depending on the severity of the compression. The symptoms experienced among patients can vary depending on the area of the spine affected or compressed. In the cervical (neck) region, symptoms may be experienced in the neck, shoulders and arms down to the fingers. In the lumbar (back) region, symptoms can be felt in the back, buttocks, thighs, knee, calves, feet and toes. The most common symptoms include:
- Dull, sharp or radiating pain
- Weakness or numbness in the extremities
- Sensation of burning or pins and needles
- Difficulty walking or standing straight
- Medical history
Assessment of symptoms, previous treatments and care. - Physical examination
A careful examination by a spine specialist for limitations of movement, problems with balance, and pain. The examination should also cover loss of reflexes in your extremities, muscle weakness, loss of sensation or signs of spinal cord damage. - Diagnostic tests
Generally, we start with plain x-ray films, which allow us to rule out other problems such as infections. CT scans and MRIs are often used to give us three-dimensional views of the lumbar spine and can help detect Foraminal Stenosis .
Non-Surgical Treatment ?
- Alternating heat/cold therapy during the first 24-48 hours
- Pain medications
Anti-inflammatories, muscle relaxers and on rare occasions narcotic painkillers - Physical therapy exercises to include: stretching, massage strengthening
- Epidural steroid injections are used two-fold, first, to relieve inflammation of the affected spinal nerve and secondly, diagnostically to confirm the correct affected level at which the pain originates from.
Surgical Treatment
When conservative care is exhausted and the patients are still in pain, surgery is a logical step to relieve the pain. Traditionally, central and lateral recess stenosis is performed open with a large incision in the skin. A laminectomy and or facetectomy are performed to release the pressure on the spinal cord. Unfortunately, this technique is invasive and leads to significant post-operative pain and recovery. With innovation and advances in technology, a less invasive surgical technique has been developed to address these painful conditions such as foraminal stenosis.
- Laminectomy
During the microdiscectomy surgeons often have to resect the bone called the lamina in order to see the affected nerve and herniated disc. Recovery from microdiscectomy can be long and with bone, resection adds to possible scarring in the area the surgeon is working. Anesthesia is necessary. - Endoscopic Foraminalplasty
Unlike traditional surgery, a small ¼ inch incision is made in the skin. Your muscles are spared and only dilated in order to gain access to the surgical site. The physician uses a working channel endoscope that allows for water and instruments to pass through the scope with an HD camera attached hat provides a superior view of the anatomy and the spinal cord. The patient is under conscious sedation alert and comfortable throughout the procedure. No general anesthesia is needed and thus lower risk to the patient. - Spinal Fusion
Spinal fusion surgery is designed to stop the motion at a painful vertebral segment, which in turn should decrease pain generated from the joint. Spine fusion when indicated should be the last options offered but can be performed effectively with advanced MIS techniques. Sometimes when patients suffer from foraminal stenosis that fails a laminectomy or facetectomy are often left with instability and MIS fusion is appropriate to provide stability and further decompress the foramen and spinal nerve.
What Is The Recovery ?
Most patients can begin getting out of bed one hour after surgery and go home shortly afterward. Activity is gradually increased and patients are typically able to return to work within a few days. There will probably be some pain after the procedure and is usually localized to the incision site. However, always consult your physician before beginning any physical work.
Always seek your physician’s opinion when it is safe to return to work. Also, light administrative duty is recommended until your physician approves of any physical demands at your place of work.
At home, you will need to continue to rest. You will be instructed on how to gradually increase your activity. You may still need to take the pain medications for a while. However, pain and discomfort should begin to reduce within a couple of days after surgery. We will discuss with you other techniques for reducing pain and increasing flexibility before you leave for home. We will also discuss with you a time frame for when you can resume basic activities such as walking, driving and light lifting, and when you can return to more advanced activities such as physical labor, sports, and yard work.